
November blog
Special Economic Zones-BEWARE!!!
follow twitter @EuropeanPowell
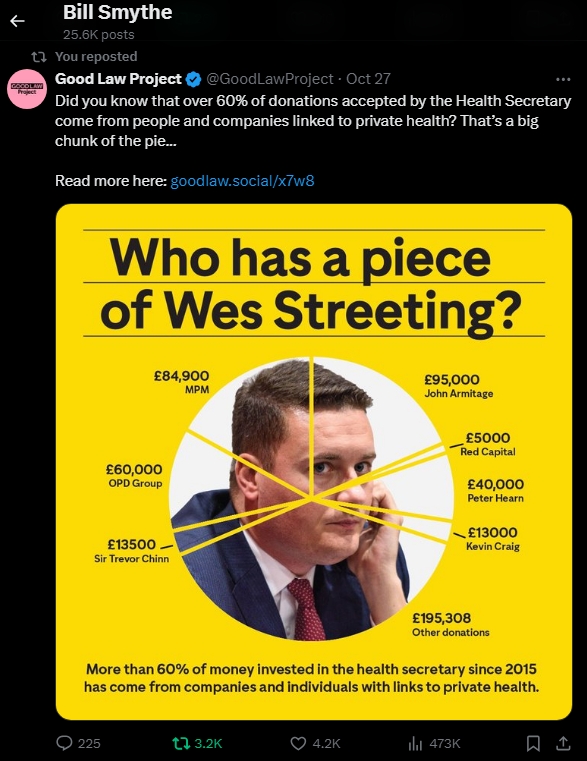
Corruption, bribes, lobbying...Wes Streeting: who bribes him?
Streeting seems fixed on several gimmicks:
1-Give every overweight unemployed worker Wegovy: means great
income for Danish manufacturer of Wegovy, Ozempic-Nordisk. Schroder Equity fund
has £10 million of Novo Nordisk shares.
Armtage, founder, funded Streeting from 2022 by £95,000 and £25,000
to Labour
Nordisk shares doubled, gaining millions for Armtages
fund
(PE 25 October)
2-Streeting also wants NHS smart watches for NHS patients-monitoring
bp, heart rate, sugar etc-at what cost? Who makes them: Infosys, Fujitsu,
Easily hacked-gps position etc
3-NHS app-easily hacked, surveying your medical data, sold to insurance companies to refuse insurance, cherry pick profitable patients...
4-Palentir, Petyer Thiel Federated data platform: data sold to anyone, hacked by Russia, Iran, given to insurance companies
Tax oil, Google, Amazon, ban tax havens, collect £37 billion from Di do, collect uncollected taxes, tax the rich same rate,
The levels of corruption, bribes, lobbying has risen above all records
Corrupt governments favour "business and industry" way above ethical, vocational frontline NHS and Care staff, working their butts off despite the government
The electorate are never informed, never asked, have no influence
Government members profit from contracts, IT "provision" (sic)
Di do Harding received £37 billion-never tracked, traced or accounted for...
The NHS and Social Care should have a simple Bevan model: "Hospitals" (not Trust Hospitals), Doctors, Nurses, Radiographers, Midwives PAID FAIRLY AND SIMPLY (look at the complexity of calculating monthly salaries, unfathonable pension rules.,..!)
Private health insurance, private hospital
chains should BE ENTIRELY SEPERATE FROM NHS (and not be given public funds to
invest or survive...)
Throughout the decades, the NHS has been the object of concealed plots, weasel words...
Thatcher and Regan wanted to "sod the poor", low taxes for the rich, privatise everything, stop opticians, dentists, private health insurance...
Blair wanted to be sweet to industry-and big businesses like private health companies.
Brown was more inclined towards the poor and the NHS
Milburn, Lansley, Hunt-all opened up our NHS to big private companies...
I would bet that Massey (ex DSHSS, now head of puppet GMC-will get a Lordship and a gong-for confusing AAs, PAs with real Doctors.
Should "Trust" Hospitals be renamed "Hospitals"-as there
is no Trust!
Allowed to purchase land for expansion, rather than forced to sell...?
In the 2000's, private corporations bough many NHS dental practices, with thousands of NHS patients, which they could convert to private patients.Centene, United Health lobby hard to be able to buy bits of our NHS-and sellout when they cannot make "enough"(humongous) profit. Gullible PMs give Stevens et al positions as "head Health Advisor" to Centene, United Health execs... Heaven help us!!!
Surprisingly, Enoch Powell was quite a sensible MoHealth, Frank Dobson-outed by Blairite successors Milburn to wreck further... David Owen David Anthony Llewellyn Owen, Baron Owen, CH, PC, FRCP was an actual Doctor.
He, and Ted Heath were the only two replies to letters about Dentistry and the NHS, from hundreds of letters...
Likewise, private for profit corporations bought up many medical partnerships premises, and leased back to GPs: they had control of the policies, selecting good profit patients, culling expensive patients, and coercing well off patients into private medical insurance policies -making profits from the NHS.
Similarly, the US style (Un)Accountable Health Organisations, (Dis)Integrated Care Boards,aim to increase profits by rationing care, culling expensive patients
as do Private Health Insurance companies by refusing treatments, co payments, top up fees, and culling difficult expensive patients, and selecting cherry picking, cream skimming easy patients.
The Kaiser Permanente model employs Doctors, owns the buildings, and sells Private Heralth Insurance.
Private health corporations should be completely separate from the NHS: Streeting-Let
them stand alone-not subsidised from NHS funds..
They do not have "spare capacity". They take NHS frontline teams FROM
our NHS.
Every qualified doctor can work in private health: surgeons can choose to do so, or emigrate:
FULL PAY RESTORATION, agreed in Scotland, is essential.
Private hospitals cost more-they have to make a profit for their CEOs, Directors, shareholders: it is their prime duty to do so...
NHS tax funds should NOT be given to private corporations, private hospital chains.
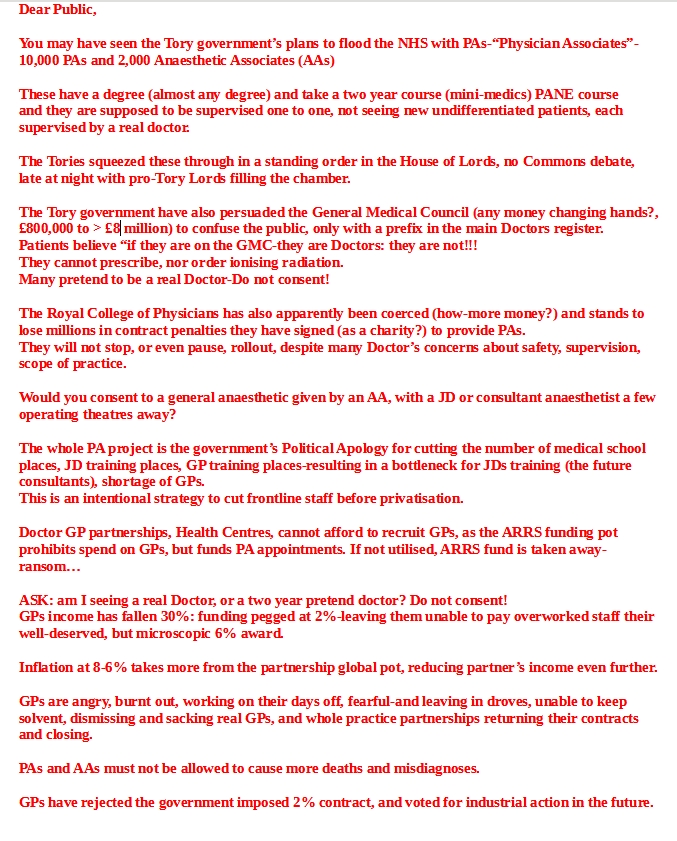
PAs should stop being promoted ahead of training for Real Doctors, GPs, with funding to EMPLOY them.
The core contract, properly funded, should allow practices to hire more GPs (not prevented by ARRS funding rules, and partners aided to recive full awarded pay
If an NHS GP is burnt out, overloaded, underfunded-it is no surprise they hand back their contract, and work privately-£60 for The London et al...
Doctors
not to be-Terrifying Guardian article on Physician Associates (Politicians
Apologies)
What if your ‘physician’ wasn’t actually a
doctor at all? Beware this new reckless experiment
Rachel Clarke
The NHS says it’s not trying to replace qualified doctors with physician
associates. But we can see the terrifying truth
Thu 20 Jun 2024
Something radical, precipitous and sweeping is under way in the NHS. It’s
untried, untested and sorely lacking in evidence, with the potential to cause
significant patient harm. I’m talking about the Department of Health and
Social Care’s project to rapidly expand so-called medical associate professions
(MAPs), the largest group of which are termed physician associates (PAs). None
of these groups have a medical degree, nor postgraduate medical training. But
their deployment in our health service is billed as “essential”
workforce planning – the only way to address rising patient demand and
a desperate shortage of trained medics.
The Independent Healthcare Providers Network (the Profiteers) offers 2.5 million
Treatments...
but want
-solid long term contracts,
-guaranteed fixed tarrifs, and
-supply of patients REJECT!!! SAME AS PFI...
no poaching NHS staff,intensive care bedsno cherrypicking
value for money CHPI
outsourcing cataracts meant many NHS eye departments unviable, but treating complex cases
reverse outsourcing by insourcing

The Great NHS Heist right click-open or select-open
Phil Hammond I'm Still a Doctor Brilliant read!!!
Tales from the past-Repeated...
Doctors Not To Be 8 March 2007 Are the careers of eight thousand junior doctors being stuffed up on purpose? The rushed implementation of the Modernising Medical Careers (MMC) programme looks like just another Labour cock-up, but its consequences are suspiciously advantageous to a Government intent on busting the medical cabal. The failure of the Medical Training Application Service (MTAS), a centrally-controlled computerised bun fight, was predictable to anyone with a passing knowledge of NHS IT programmes. It was flawed in its content, an unvalidated bullshitters' paradise that has allowed erudite disaster zones to get jobs at the expense of much better doctors, and flawed in its delivery. Making so many doctors apply at the same time was bound to lead to persistent crashing of the site, lost applications, interviews offered for specialities not even applied for and interviews at both ends of the country on the same day. The Government has been able to ignore earlier concerns that the new system was unfair and unworkable, safe in the knowledge that doctors are finding it hard to get public sympathy. Greedy GPs and consultants, rather than privatisation and target-chasing, have been cleverly fingered as the prime cause of NHS debt, and junior doctors bleating to the media that they may have to become lawyers, work in the City or move to Australia will have Patsy Hewitt chuckling in her cornflakes. The shit has finally reached the fan, thanks to West Midlands surgeons suspending their junior appointments, but health minister Lord Hunt was unfazed: ‘MMC was devised with the help and support of the Royal Colleges, the Academy of Medical Sciences and the BMA.’ So it's all their fault. But what's in it for Labour? Having acknowledged they were stuffed by the BMA over consultant and GP contracts, the Government – having increased doctors' numbers – now wants to get by with as few as possible. Doctors have priced themselves out of the market, so medicine is being broken down into simplistic tasks that can be hived off to private companies employing lowest common denominator health workers. Having 30,000 junior doctors compete for 22,000 jobs creates sufficient anxiety and insecurity for those with a job to work illegal hours covering holes in the NHS without whistle-blowing. Junior doctors aren't going down without a fight (support them at www.remedyuk.org) but is seems unlikely that enough would resign en masse to panic the Government. A more likely scenario is that they'll cancel their memberships of the BMA and Royal Colleges, a situation that would delight Labour. The GMC has already been stuffed by Liam Donaldson's ludicrously bureaucratic re-licensing plans, and taking out the rest of the medical establishment would make doctors even easier to control. The Department of Health has announced a review of MTAS, but not suspended it. Thousands of juniors have joined up at Remedy UK, and are planning a protest on March 17 from the Royal College of Physicians to the Royal College of Surgeons. But to get public and media support, doctors need to explain how their personal misfortune will affect patients. For the NHS to thrive, it has to ensure the best and brightest doctors are given the right jobs. MTAS doesn't appear capable of ensuring this. When I'm finally dragged kicking and screaming into an NHS ward, I want to be treated by a doctor with sufficient wisdom, skill and motivation to do the job properly, not a dumbed-down generic health worker reading from a guideline. Cutting down the supply of good doctors may well balance the NHS books in time to save Hewitt, but the long-term consequences will be dire for patient safety.
What Should Gordon Do? 15 June 2007 What should Gordon Brown do with the NHS? He may want to put his ‘unique stamp’ on it, but Blairites are working around the clock to progress the market reforms beyond the point of no return. The great con of Blair's NHS was to preach the rhetoric of patient power whilst handing over control, and a vast sum of public money, to the private sector. To argue that this is not privatisation of the NHS is nonsense, but then Blair excelled at that. The tipping point for the NHS will come if Labour pushes through its plans to outsource up to £64 billion worth of commissioning to multinational corporations such as United Health. This would suit Blair's friends at McKinsey, who can charge a fortune to the NHS for brokering the deals and also represent many of the US companies who stand to gain. At least one senior executive at McKinsey has a staff pass at the Department of Health. In return, Blair will have ample boot-filling opportunities in America. In Blair's absence, Patsy Hewitt is rushing through his agenda before her exit, aided by David ‘Nibbler’ Nicholson, the surprise choice as NHS chief executive, who leapt up the shortlist after a meeting with Blairite health guru Professor Paul Corrigan. Nicholson in turn has appointed an NHS management team that is putting intense pressure on strategic health authorities and PCTs to outsource their commissioning. The idea that PCTs will retain ultimate control (and hence keep the NHS public) is a myth. So what is Brown to do? Clearly a return to the Old Labour Stalinism of diktat by bureaucracy is impossible. And yet Blair's model is equally didactic, suggesting market competition is the only way forward and peppering it with promises of choice, when patients only get to choose what the Government (or United Health) wants them to. The junior doctor selection crisis is the most extreme example of this – thousands of doctors who have worked for seven years or more in the NHS are allowed only one choice of job, in many cases only specifying a region (e.g. Scotland) rather than a hospital unit. Stalin invented the internal market, the Tories introduced it to the NHS and Blair is polishing it to imperfection. The NHS works because it is a one-stop shop – once you're in it, you get all the care you need. Contrast this to America, where patients who have brain tumours removed are sent home the next day if the insurance package does not include continuing care. If American managed-care corporations unleash their ‘expertise’ on the NHS, only an American system can result. Profitable patients are cherry-picked while unprofitable patients are dumped. Brown must reverse this without seeming to be Old Labour. The solution is to deliver what Blair and Hewitt have pretended to promise: ‘a devolved NHS where 80% of the decisions are made locally’. Working in the NHS is like pulling people out of a river without bothering to look at who's pushing them in. If Labour really wants patients to get involved in shaping services, it has to move the money upstream and stop the dysfunctional schism between top-down marketing and local decision-making. Most NHS resources now go on managing chronic illness, and many patients manage themselves perfectly well for all but three hours a year, when they're hanging round the surgery or outpatient clinic. Tapping into this expertise and getting patients to help other patients in their communities is the best hope of stopping the log-jam downstream. The message is simple. Local partnerships between patients and NHS staff work, market reforms don't. But will Brown swallow it? 10 www.plosmedicine.org May 2005; Volume
so much money has already been wasted on NHS change that he'll
have a job convincing the staff of the need for more. He's proposing polyclinics
to do much of the work done in district general hospitals, but we've already
invested £1.4 billion in Independent Sector Treatment Centres that were
supposed to do the same. ISTCs were encouraged into the market with guaranteed
contracts paid above tariff. Last year, they were paid for 50,000 more operations
than they carried out. The vast majority of waiting-list reductions were carried
out in existing NHS hospitals and a huge sum has been wasted on unnecessary
competition. The NHS already has a competitive market under Payment By Results.
Or rather activity. Hospitals can only survive by sucking as many patients as
possible through their doors. ISTCs couldn't attract the custom, not least because
they failed to submit sufficient outcome information to the Healthcare Commission
to enable them to be audited for quality and safety. Polyclinics may well have
the expertise to treat patients closer to home but whether they can stand up
to the might of desperate hospitals remains to be seen. To get the support of
NHS staff, Darzi doesn't just need to consult them, he needs to publish evidence
showing his reforms would work. The Academy of Medical Royal Colleges has performed
the most comprehensive review of the reconfiguration plans and agrees that highly
specialised services such as major trauma, heart and brain surgery need to be
specialised on fewer sites. But it found no evidence to support the centralisation
of the non-complex, high-volume work done in district general hospitals. There
is, however, evidence that patients feel access to GPs has improved in the last
few years, which makes Brown and Darzi's peculiar focus on extending opening
hours puzzling. The review smells strongly of hastily assembled populist opinion.
Clinical medicine has been reformed in the last twenty years by focusing on
the evidence, not the expert. The same needs to happen with NHS reform. Don't
change the system until you can prove you've got something better.
IT expert put it: ‘Scotland and Wales are smaller communities, with more
collaboration and co-operation than the market-obsessed English NHS. They assume
that NHS staff are generally trustworthy and have developed ‘higher trust’
IT systems that are simpler and easier to access, and have managed to gain the
consent of patients. Contrast this to England, where no-one can be trusted and
the media is paranoid about leakage of confidential data. So you've built hugely
complex programmes with military grade security to block the few bad people
but which take ages to log onto, navigate around or swap user. At their worst,
they stop you practising medicine, rather than enable you to do the job better.’
Granger's parting shot from the IT programme was to boast at how tough his
More Staffing Problems 8 April 2009 A key question for the investigation into the appalling standards of emergency care at Mid Staffordshire hospital is: ‘Why did no member of staff blow the whistle sooner?’ In a 2006 Healthcare Commission survey, only 27% of the Mid Staffs staff said they would be happy to be treated in their own hospital, a powerful indication that standards were unacceptable. And after Bristol, the General Medical Council deemed that doctors had a duty to speak up when the service becomes so unsafe that patients are being harmed. However, the experience of Dr Rita Pal in nearby North Staffs suggests that whistle-blowing in the NHS remains a thankless task. Dr Pal identified serious shortcomings in the nursing and medical care of patients on Ward 87 of City General Hospital, Stoke on Trent, when she started working there in August 1998. These included a lack of basic equipment such as drip sets, a lack of adequate support and supervision for junior doctors, a gross shortage of staff and repeated ‘do not resuscitate’ notices. As a result, patient care was often poor, with a lack of baseline observations and routine blood tests, and there appeared to be an unacceptably high mortality rate. In November 1998, Dr Pal articulated these concerns to senior nursing and medical staff, and put them in writing. As a result, she was bullied and victimised. She was wrongly accused of causing a needle-stick injury and inserting the wrong date on a drug sheet, and she found out that her previous consultant had been contacted to ascertain whether she was ‘capable of doing the job’ (i.e. flying by the seat of her pants with inadequate support and resources, surrounded by hostile nursing staff and patients dying unnecessarily). She requested leave because she (quite reasonably) felt unable to care for patients in this environment. Subsequent investigation found that Dr Pal's allegations had been spot on. A review in May 1999 by Mrs T Fenech from the Infectious Diseases Unit found ‘serious deficiencies in nursing practice’ and that ‘the level of care demonstrated for some patients on the ward at the time of my audit was nothing short of negligent.’ In 2001, an internal report concluded that the directorate failed to take appropriate action when the allegations were made by Dr Pal and that patients had suffered from poor standards of care. And in March 2002, the Commission for Health Improvement still found ‘serious deficiencies’ particularly with ‘the level of supervision, workload and work patterns of junior doctors working within medicine.’ So not only were Dr Pal's initial allegations accurate, but four years later very little had been done to address them. Dr Pal took her concerns to the General Medical Council and – eleven years after first raising concerns – is still embroiled in a fight to ascertain the true extent of the harm done to patients on Ward 87. A mature and safety-conscious NHS would have thanked her for raising concerns to help improve patient care, and acted on them. Instead, she has been bullied, falsely accused of malpractice and repeatedly denied access to key documents to help support her case. Last week, Sir Ian Kennedy, retiring chair of the Healthcare Commission, spoke of the bullying culture in the NHS that still ‘permeates the delivery of care.’ Those who are brave enough to speak up about deficiencies in care are being pilloried and silenced. In such an environment, patient safety can never flourish. Dr Pal has lobbied (via her MP Andrew Mitchell) for the Commons Health Select Committee to investigate the problems faced by whistle-blowers in the NHS. She has also started a support network for whistle-blowers and can be contacted at: dr.ritapal@googlemail.com Struck Off and
Labour's Pains 24 June 2009 New health secretary Andy Burnham does a fine line in cheesy tributes, describing his predecessor Alan Johnson as ‘the postman who delivered for the NHS.’ But Johnson got out just in time, leaving Burnham (39, Capricorn) to pick up a number of suspicious packages: The swine flu pandemic, a predicted Summer heat-wave, a staffing crisis caused by the 48-hour week for junior doctors and a projected five-year shortfall in NHS funding of £20 billion. Alas, his maiden speech at the NHS Confederation conference did little to inspire confidence: “Can we do more to get through the challenge and to the next level, going from good to world-class?” He also promised to “unlock the 1.4 million people working in the NHS” and “create a truly people-centred NHS – which genuinely empowers patients and carers as experts potentially backed with control over funds, moving on heath promotion and physical activity, helping people to lead full happy lives, working with public sector partners to wrap care around patients and to place quality at heart of everything”. Burnham is clearly au fait with new Labour bullshit, but can he stop the NHS going tits up in the recession? The NHS has undoubtedly got better over the last decade, but there are still huge variations in the quality of care, and plenty of commercial secrecy and petty rivalry disguising poor practice and waste. Lord Darzi has been frantically encouraging doctors to get more involved in management, and it certainly makes sense for a clinical service to be run by clinicians. But the English NHS is stuck with a market which hasn't delivered a good enough service because nobody knows how to spend £100 billion a year without wasting half of it. The solution was supposed to be word class commissioning (WCC), a phrase dreamt up by Mark Britnell, the self-styled NHS director general for commissioning and system management. Britnell also came up with the FESC framework to encourage the private sector to take control of the purse strings. Britnell was the golden boy of the department of health, voted third most influential person in the NHS by the Health Service Journal, a chief executive in waiting. Until he jumped ship this month to join KMPG, one of the companies involved in FESC. The revolving door from NHS policy maker to the private health provider is hardly new (Simon Stevens, Alan Milburn, Patricia Hewitt, Lord Warner, Baroness Jay, etc.) but for Britnell to time his escape as Burnham arrives does not bode well for the NHS or for Burnham.
and here is how Allyson Pollock described it back then:
“The Darzi report is simply a glib advertising campaign on behalf of the
healthcare industry and a new generation of greedy healthcare entrepreneurs.”
If you’re not familiar with Allyson Pollock, she is a Professor of Public Health and NHS campaigner who predicted many of the problems we see now in the NHS, and much of the expansion in privatisation which has occurred in recent years. I trust Allyson, and so I’m nervous to see Lord Darzi placed in a position of prominence again. I’m not only nervous however, but confused. I wrote a newsletter several months ago explaining that there was a huge amount of concern about the low productivity in the NHS at the moment, and about the two separate reviews that had been started to investigate the problem.
Why is he focusing on this issue first, when he could be focusing on emergency investment into the crumbling NHS hospital buildings, or providing immediate support to the NHS workforce? And why is he involving Lord Darzi?
Concerningly, I suspect it is because Starmer’s Labour party have already decided they want to reform the NHS through the involvement of private companies, and they need a report to back up their plans. Politicians are incredibly adept at deciding on the answers they would like from reports like these, and then approaching the “right” people to write them, and on this occasion Lord Dazi appears to be the right man.
Further bios of Hunt, Javid, Coffey, Barclay, Atkins cwould show a desire to beat the BMA, and Doctors, into a pulp by forcing PAs, AAs into subtitution of real qualified Doctors...
We will have to watch Starmer, Streeting, and their allies from the Blair / Brown era closely. Many people defend Tony Blair’s record for the NHS because he brought down the NHS waiting lists, but he and his team did so while wreaking havoc on the infrastructure of our health service. Their Private Finance Initiatives (PFI) left many NHS trusts with enormous debt, costing the taxpayer billions; the final debt not set to be paid off fully until 2050.
We finally have a chance for a fresh start after 14 long years of Conservative governments undermining the NHS. This opportunity to turn things around should feel fresh too; it should not be a rehash of old plans – plans that didn’t help patients, and which put a lot of money into the pockets of private company shareholders.
We need things to improve, not change, and we don’t need any more NHS privatisation!
I’ll keep you up-to-date as things develop… Phil Hammond
Real NHS leaders In the thick of it...
Palantir’s, Thiel, federated data platform, can easily be sold by a desperate bancrupt government to private health insurers, used to eliminate expensive risky patients, sell insurance to low risk patients, exclude patients from GP lists, show which patients are high risk of admission to hospital-expensive
Risk of blackmail: if you do not take wegovy, you get no benefits
Streeting is a Jekyll and Hyde character- like all politicians..
"Change"- they can do anything…
Bribed by private health companies
Speeches to alarm- the NHS is broken
Needs reform
Milburn
Outsourcing
Any Qualified Provider
no ten year workforce plan
PAs
Darzi: we already know what’s wrong
Believe Marketisation-or you get no promotion
Kaiser Permanentecompared with NHS-used bad statistics-but now Government policy
Dissolve all the good things-Strategy planning, public health policy, don't
collect statistics